

BACKGROUND
GVHD remains a major cause of morbidity and mortality after allo HSCT. The past few years have shown a number of successful advances in cellular therapies for the treatment of hematologic malignancies. It is logical to expand the use of these therapies earlier, in strategies aimed at prevention. Several studies showed that regulatory T cells (Treg) can reduce the incidence of aGVHD.
METHODS
Studies were identified using electronic databases (Medline, Embase, and Cochrane). Preclinical studies were excluded. Data analysis was performed using GraphPad Software 8.4.2.
RESULTS
160 patients were identified from 7 clinical studies. 85% of the patients had acute leukemia and were in complete remission at the time of transplant. Tregs were isolated from either UCB or PB. Tregs were expanded ex-vivo using IL-2, CD3/CD28 ab coated beads and K562 cells in three studies (n=40).
1.Ex-vivo expanded Treg: In a phase I study (Brunstein et al) of UCB-derived Tregs in 23 pts undergoing double umbilical cord transplantation, Tregs were cultured with antiCD3/anti CD28 and IL-2. Ex-vivo expanded Tregs were given on day+1 and day+15. Eighteen pts received Treg cells at dose of >3x106 cells/kg. Grade II-IV aGvHD was seen in 39% of pts who received ≥3x106 cells/kg vs 43% in historical controls. In this study, CsA+MMF or sirolimus+MMF were used for GvHD prophylaxis. In a follow up study of 11 patients, Tregs were markedly expanded using K562 cells. Higher Treg doses were achieved up to 100x106cells/kg and the median proportion of CD4+CD127-FOXP3+ within the infused products was 87%. Grade II-IV aGVHD was 9% at 100 days vs 45% in control group. Treg cells were not detected in the peripheral blood after 14 days of infusion. In a phase II study (Kellner et al; Zeng et al), three of six pts undergoing PB MUD received ex-vivo expanded UCB-derived Tregs 1x106/kg at day-1. All developed aGVHD due to the high donor Tcon cells in the graft with donor Tcon:UCB Treg ratio as high as 356:1. Sixth patient was given 1x107 cells/kg Tregs in the presence of anti CD3/28 microbeads and IL-2 with Treg:Tcon ratio of 1:40. No aGVHD was observed in this patient compared to the others who received Treg at the dose of 1x106cells/kg.
2.Unexpanded Treg: In a study (Di Ianni et al) involving 26 high risk leukemia pts undergoing haplo-transplant with TBI based conditioning, 21 pts were infused with donor Tregs at a dose of 2x106 cells/kg and five pts were infused with Treg at a dose of 4x106 cells/kg on day -4, followed by Tcon infusion ranging from 0.5x106 to 2x106 cells/kg on day 0. No post-transplant immune suppression was given. Grade II-IV aGVHD was observed in 2 out of 26 patients who received 4x106cells/kg Tregs and 2x 106cells/kg Tcons. No GVHD was observed in pts who received 2x106cells/kg Tregs followed by 0.5-1x106 cells/kg Tcons. A phase II study by the same group (Martelli et al) reported on an additional 17 pts who received Tregs (2x106cells/kg) at day-4 co-infused with Tcon (1x106cells/kg) at day 0. Six of 41 (15%) evaluable pts developed grade II-IV aGVHD (vs 11% in historical cohort) with two pts requiring a short course of immunosuppression. Incidence of relapse was lower in Treg group than historical controls (5% vs 21%). In a phase I/II study (Meyer et al), 12 pts with hematological malignancies who underwent HLA-matched transplantation received purified Tregs (1-3x106cells/kg) on day0 followed by Tcon (1-3x106cells/kg) on day+2. GVHD was seen in 80% of pts with 50% being grade III in pts who received frozen Tregs. Upon revising protocol, 7 pts were given fresh Treg. The patients also received either tacrolimus or sirolimus for immunosuppression. None of 7 pts in revised cohort developed GVHD. Recent study applied hyper-fractionated TBI to the conditioning regimen in 12 pts out of 40 to further reduce leukemia relapse in Treg/Tcon based haplo-HSCT. Treg was administered at the dose of 2x106cells/kg and Tcon at 1x106cells/kg. No post-transplant GvHD prophylaxis was given. Grade II-IV aGVHD was observed in 12 pts.
CONCLUSION
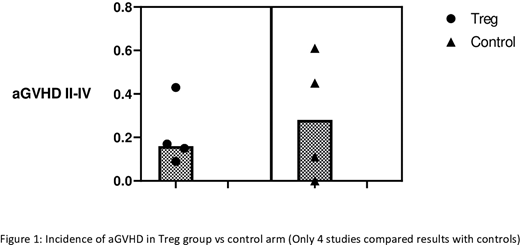
These studies suggest that Treg therapy may represent an effective prevention strategy against acute GvHD (figure 1). Stimulated Treg expansion strategies and higher doses of Treg appear to be associated with lower incidence of aGVHD. Treg infusion was well-tolerated without serious adverse events. Large prospective clinical trials are warranted in order to establish the optimal infusion dose, optimal expansion strategies and dosing schedule.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal